

Anterior cruciate ligament (ACL) rupture
What is it?
The ACL is one of the four main ligaments of the knee. A ligament is a fibrous band that connects two bones together across a joint with no muscle attachment.
Ligaments have two main roles. The first is to guide the movement of a joint by their bony attachments and the second, possibly greater role, is to send information via their nerve endings to the brain about the position of the joint. The brain uses this information to recruit muscle activity to control the joint. (This is known as proprioception).
The ACL runs obliquely through the centre of the knee from the back of the thigh bone to the front of the shin bone. Its main function is to stabilise the knee particularly on twisting or pivoting activities. It is therefore particularly important during most sporting activities but also surprisingly necessary during more mundane daily activities.
How does it rupture?
The ACL is typically ruptured with a twisting motion on a rather straight knee. A non-contact pivot or side step at soccer or rugby, deceleration and twist at netball or slow speed twist while skiing are common stories. The injury may be accompanied by tears to the cartilages, joint surface damage or be part of a multiligament injury.
Occasionally the ACL can rupture with minimal force or energy causing a delay in the diagnosis.
Symptoms
The initial symptoms following an ACL rupture are of the acute injury. There is usually acute pain often accompanied by a feeling of a pop or tear. Swelling develops fairly rapidly due to bleeding into the joint and the knee will often buckle on attempted standing. There may be difficulty bearing weight.
Following recovery from the initial injury the swelling and pain will usually settle. A feeling of instability or untrustworthiness is the main ongoing complaint with occasional true giving way or buckling of the knee particularly on twisting or uneven ground. Further swelling and pain will accompany these episodes and further structural damage can occur within the joint.
Often symptoms will only occur on attempted return to sport.
How is it diagnosed?
The diagnosis of a ruptured ACL is almost entirely from the description of symptoms and the examination of the knee joint. Increased forward translation of the shin bone on the thigh bone is detected by the Lachman test picture and a further test of rotation of the joint called the pivot shift test will reproduce the unstable feeling on twisting activities.
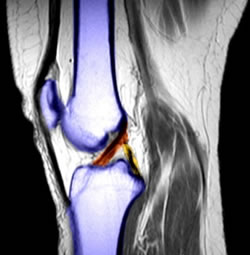
The diagnosis may be confirmed by an MRI scan and an Xray is usually taken to exclude associated bony injury.
What is the treatment?

Treatment will initially focus on recovery from the acute injury with Rest, Ice, Compression and Elevation (RICE). Painkillers and anti inflammatories will undoubtedly also be necessary.
The subsequent treatment of a ruptured ACL will depend upon the aims, activity profile and ongoing symptoms of the individual. In general, any persistent instability of the knee will lead to further damage initially of the cartilage and subsequently the joint surfaces. It is therefore important to avoid further episodes of this instability. If this cannot be controlled by avoiding certain activities or refraining from sport, then a reconstruction of the ACL should be considered.
ACL reconstruction
A reconstruction of the anterior cruciate ligament involves removal of any remaining original ligament fibres and their replacement with graft tissue taken from around the knee. The operation is done using keyhole (arthroscopic) surgery and may be done in combination with other procedures if necessary.
There are two common graft types used to reconstruct the ACL: the hamstring tendons and the patella tendon. Using modern arthroscopic techniques the results for each graft are comparable and the choice will depend upon the activities and often the occupation of the individual.
Bristol
Contact us on
0117 980 4037
or
0117 980 4046